
by American College of Surgeons

Major metropolitan areas such as New York, Seattle, and Detroit have dominated news of the COVID-19 outbreak, but rural hospitals and health care systems must also prepare for a surge of coronavirus patients. Surgeons at one rural health care system on both sides of the New York-Pennsylvania border have reported on their preparedness response plan for dealing with the COVID-19 surge in an “article in press” appearing on the website of the Journal of the American College of Surgeons ahead of print. This rural surgery plan takes into account challenges unique to a rural population and geography, and it includes greater utilization of telehealth and coordination of resources and communications at affiliated centers spread over a large geographic area.
“We have an older patient population, and they have more comorbid conditions than what you might find in an urban area,” said Jean Miner, MD, MHA, MMEL, FACS, a general surgeon at Guthrie Clinic/Robert Packer Hospital in Sayre, Pa., and article coauthor. “Our population is also very spread out, with about 77 people per square mile, and some of the research shows that up to 35 percent of the people in rural areas don’t have Internet access. Some of our staff doesn’t even have Internet access.” By comparison, New York City has about 27,500 people per square mile.Robert Packer Hospital is a 267-bed tertiary care teaching hospital in Sayre, a town of about 5,400 people, 270 miles northwest of New York City. It is the primary institution of the Guthrie Clinic, a nonprofit system of five hospitals that serves an area of about 770,000 people in 12 counties in northern Pennsylvania and the southern tier of New York State.”Our older patients are at risk of not only complications from COVID-19 and the higher mortality rates, but also have chronic diseases that we must also take care of to try to keep them out of the hospital at this time,” Dr. Miner said.
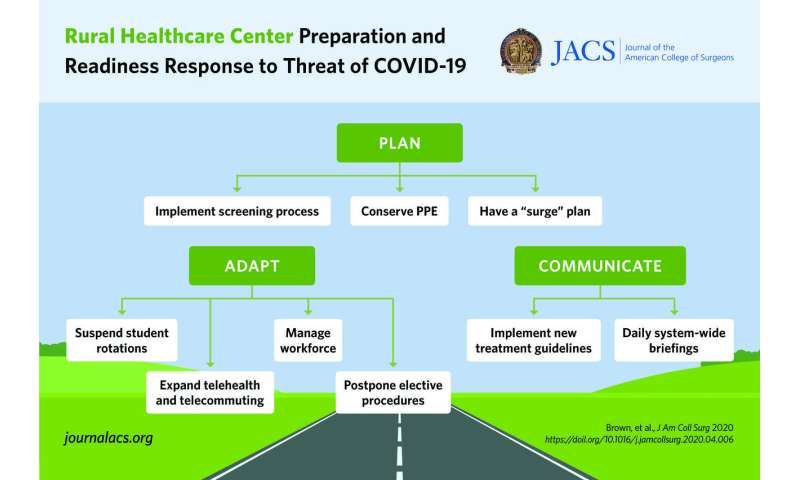
Key components of the preparedness plan include:
- Implementation of a screening process for visitors and employees (which began in early February) and tightening that process as more information about the coronavirus became available
- Having nonessential staff work at home before such a mandate was in place from governors in either state
- Conserving personal protective equipment (PPE)
- Postponing elective procedures
- Having a contingency plan to redeploy a pool of volunteer physicians and advanced practitioners to cover areas where they’re needed during a surge of COVID-19 patients
A centerpiece of the response plan is a rapid expansion of telehealth. Like many health systems, Guthrie Clinic has limited the number of in-person clinic visits. With the recent approval for telehealth expansion by the Centers for Medicare and Medicaid Services, Guthrie Clinic saw its number of providers participating in telehealth soar from 12 before the COVID-19 outbreak to 252 providers performing remote office visits and 450 having access to the platform after the outbreak began.
The telehealth system works despite the limits of Internet access in rural areas, explained coauthor Burt Cagir, MD, FACS, a general surgeon. Most outpatient clinics within the system have telehealth kiosks, and the system is flexible to fit each patient’s needs. “We allow all of our patients to communicate with any and every modality available to them, such as cellphones so they’re able to do video conferencing,” he said. Landline telephone calls are also handled and documented in patient records. The system now has the capability to do 1,000 video visits daily, he said.
Another important element of the response plan is what Dr. Cagir called “the patient safety huddle” first introduced in 2016. Senior leadership staff meets for a half hour each weekday morning to review patient safety issues. By 2018 a second huddle was added to identify trends from the previous day or week and to extrapolate forecasts for the next day or week. “We converted our forecasting and trend huddle to a COVID-19 huddle immediately in February, and the patient safety huddle system became the patient safety and personnel safety huddle,” Dr. Cagir said. Huddles were added for Saturday and Sunday.
Dr. Miner explained the huddle works on four staffing levels: front-line, department, hospital, and systemwide.
Joseph Scopelliti, MD, a gastroenterologist and president of Guthrie Clinic, explained that for the huddles to work effectively, they must be blame-free zones. “It means that everybody has to expose their challenges, so the second series of huddles we have every day is the patient safety huddle,” he said. “Think of it as the huddle where you have to answer the question, ‘What is impeding you from doing your job today?'”
Dr. Cagir explained that the processes the Guthrie Clinic adopted were developed using the Lean Six Sigma and the PDCA cycle (for plan, do, check, act) principles that industry has used to improve efficiency and quality.
“Without a doubt this approach is scalable to every urban and rural center,” Dr. Miner said. “Frequent communication has been key.” She noted that staff gets a daily e-mail with that day’s news, trends and expectations and that there are multiple ways staff can exchange ideas, including a Workplace from Facebook portal.
American College of Surgeons